
It has been so concerning recently to see so many posts where people are really angry and say they have had an inhaler swap. When you explore a little bit more you find out that it is not actually an inhaler swap.
We all have our preferred device, and brand of medication which can differ from others as we are all individuals.
I wanted to take some time to explore this issue some more. “Inhaler swap” has become a bit of a buzz word in the asthma community just now and this is because there has been a big push to move away from the Ventolin pressurised Meter Dose Inhaler (pMDI) which is found to be very pollutant compared to other pMDI’s in the market. In conjunction with this there has also been a push to move away from pMDI’s due to the high rate of poor inhaler technique and also the difficulty to actually have good technique. Dry powder inhalers (DPI) are now being pushed as the inhaler type people should be using.
Why are the inhalers patients are being prescribed changing?
We as a population have never been so conscious about the environment. We are on a shaky peg with it and the effects of pollution and global warming are clear to see with hotter summers, and colder winters. We need to do all we can to stop the damage getting worse. The healthcare industry is not the most environmentally friendly as there are so many single use items, items wrapped in plastic to ensure it is sterile, travel to hospitals and appointments, waste medication etc so we are looking for ways to reduce the carbon footprint and protect the environment. All specialties are doing this and in respiratory the focus has been on inhalers and which ones are better and have a lower carbon footprint. This is why there are all these swaps around.
There has been a huge issue in England (it is happening else where too) with some GP surgeries doing blanket swaps and changing all their patients from one type of inhaler to a different one. To make matters worse they are doing this without anything being said to their patients. The first a patient finds out if often when they open the bag once they have collected their prescription from the chemist. Understandably people are very angry about this and taking to social media. Initially when people were first posting about inhaler swaps this was because the device was being changed which changed the delivery method of the drug. A change of type of inhaler say from pMDI to DPI is a big issue as the technique changes and not all people have the inspiratory strength to use a DPI. This is an inhaler swap as the medication is the same, but sometimes the dose in the inhaler is different so you need to take a different number of actuations, the method of delivery is different eg pMDI to DPI.
The term inhaler swap is now being used by more people when they may not actually have an inhaler swap. It is important to understand what you have been prescribed. Have you been prescribed an inhaler using the brand name or the medication name. If you are prescribed for example salbutamol 100mcg the chemist can dispense any brand of salbutamol as long as it is a pMDI and 100mcg per actuation whereas if you are prescribed an inhaler by brand name for example Ventolin 100mcg the chemist has to dispense the Ventolin brand.
In the UK the recommendation is for all inhalers to be prescribed by brand however this is not happening. Prescribing by brand ensures the patient has security about their inhaler, they are using an inhaler they are used to , adhere to it and their technique is correct. The UK now recommends that patients should be prescribed and use the IVAX brand Salamol as their rescue inhaler not GSK’s Ventolin.
It is important to remember that all inhalers go through rigorous testing to ensure that they are fit for purpose. There have been a lot of people on social media saying that when they got a Salamol inhaler it didnt work and their asthma was bad but they found a Ventolin which corrected their symptoms straightaway. I find this really tricky to understand as the drug is the same, the dose is the same it is just the brand that is different. The would not have been able to bring Salamol to market if it was not as effective as other brands of salbutamol. I wonder if perhaps people don’t like change and there is a nocebo effect occurring.
I have also seen many comments on social media to say that they have had inhalers changed as a cost cutting exercise. You can access the cost of inhalers on the BNF website. pMDI’s which have a lower carbon content and are more environmentally friendly are actually more expensive so it is not a cost cutting exercise.
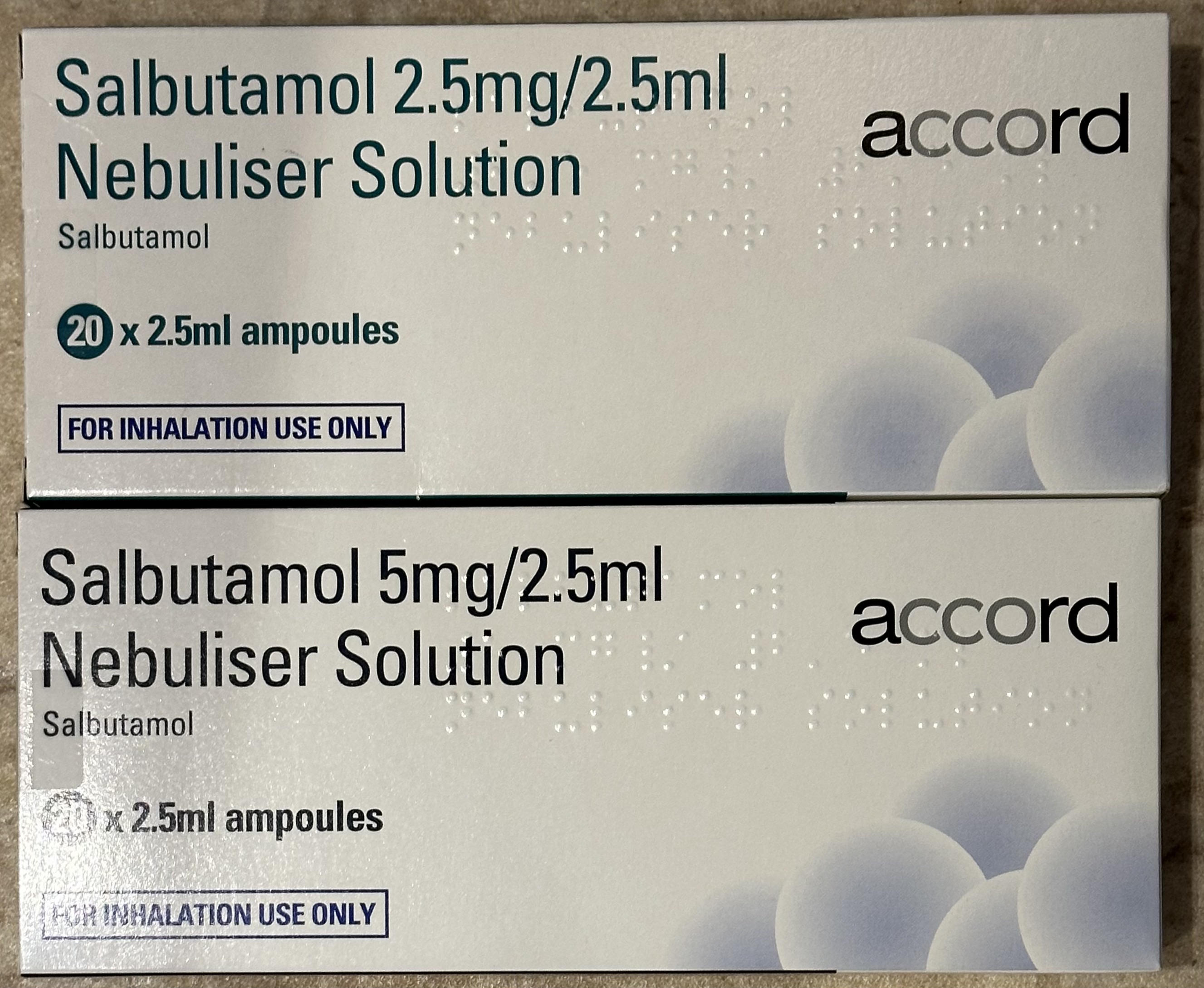
I have a lot of items on my repeat prescription so I wanted to demonstrate a couple of things which show how something is a swap or is not a swap.
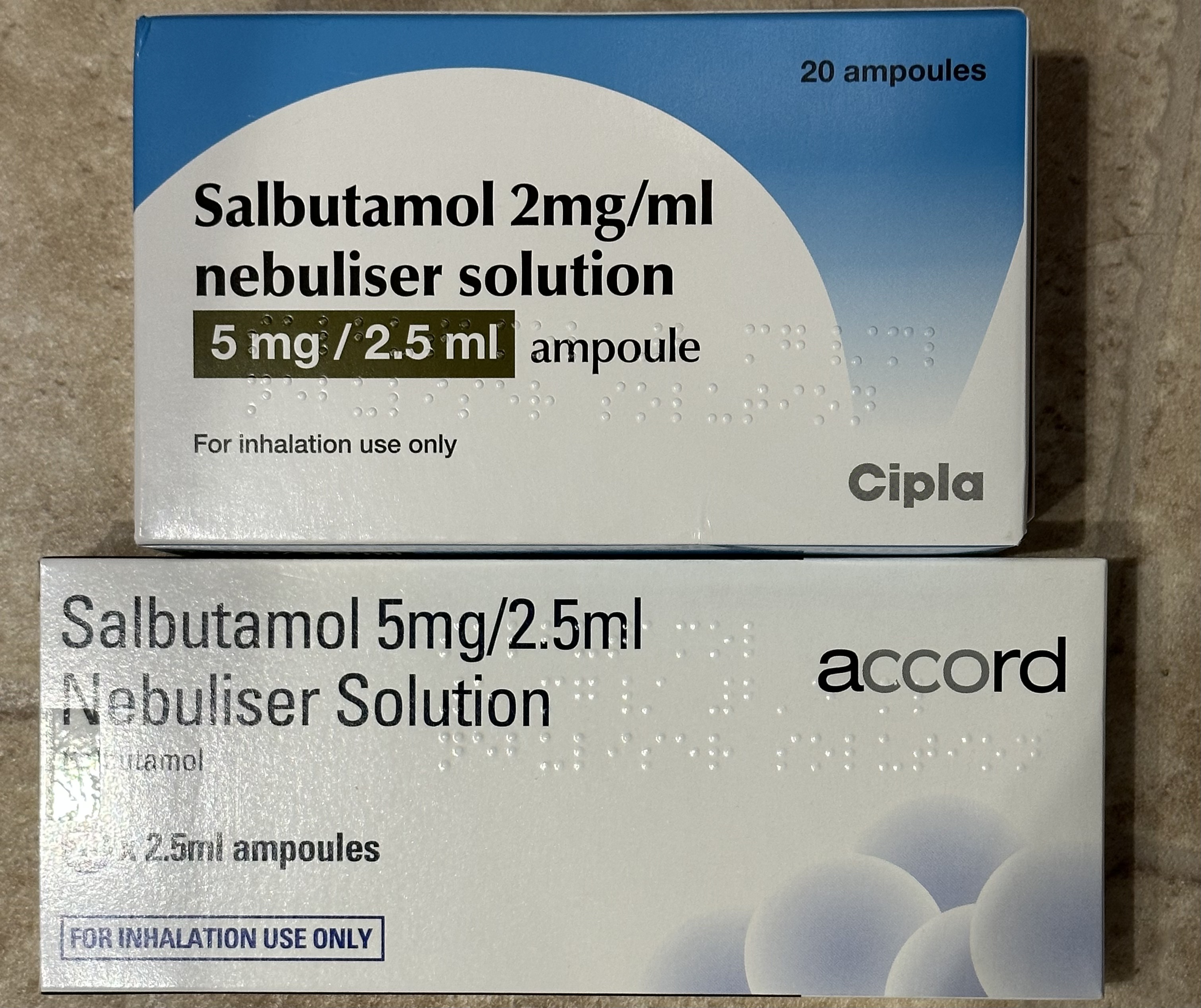
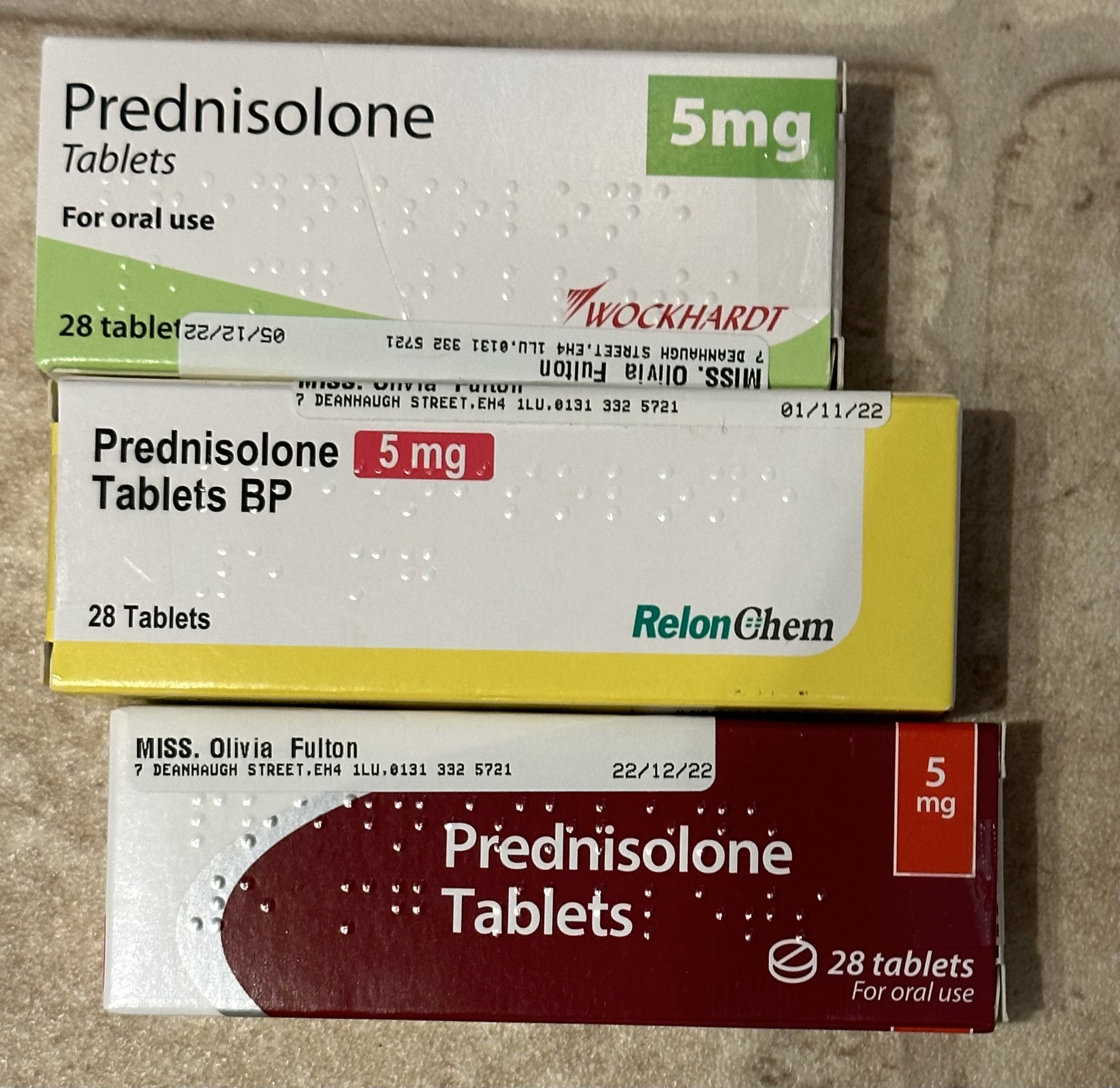
You might find similar situations with tablets and each time you pick up a prescription you might be given a different the same medication but in different boxes. This is the same type of thing as being given ventolin or salamol when the prescriptions says the medication name.
It is important for medics or anyone who is prescribing to communicate what they are doing with their patients. If there are any changes being made you need to speak to the patient to make sure they understand what is happening and why, then they need to be shown how to use a device if there is a change too.
Key take aways
- Check how your medication has been prescribed
- Make sure what you have received is the same drug, same dose, same method of delivery no matter what the brand that you have been given.
- If your prescription just says the drug name and method of delivery then you can be given any brand of that drug. This is not an inhaler swap if you get a different brand
- If your are prescribed a specific brand then you can only be given that brand for example Ventolin or Salamol
- No brand is more or less effective than the other. Each brand is tested to ensure they give the same result for the patient no matter what brand they use.
- Ask your GP to prescribe a specific brand of inhaler to ensure you get the one you want
- If you used to have a pMDI and have been given a DPI this is an inhaler swap as the technique to use it is different and often the dose per actuation varies too.
- If none of the above have occurred then perhaps ask your GP if they are bringing in any changes to their inhaler prescribing and if they are then you want to have this specific inhaler.
Ultimately this could all become redundant if patient education in asthma improves, so patients know what they are doing, know their triggers and have an action plan. This will reduce the use of reliever inhalers, reduce the need for emergency ambulances for asthma, and reduce hospital admissions all of which reduce the carbon footprint. Until patient education is improved then nothing will positively change.
